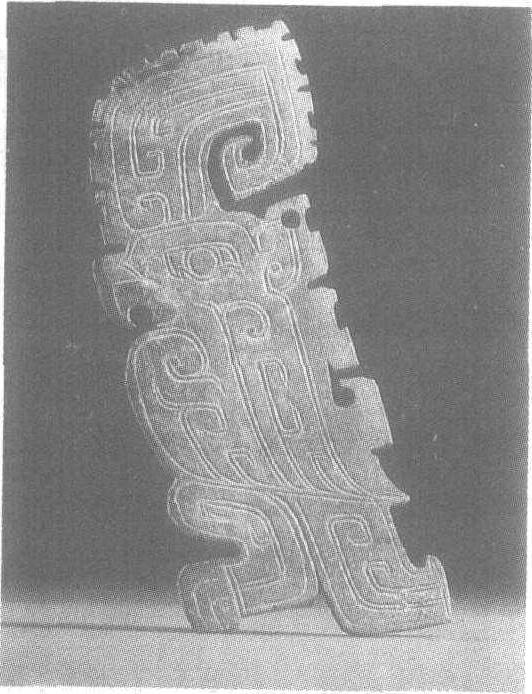
玉鹦鹉
商。高11厘米,厚0.3厘米。河南省安阳市殷墟妇好墓出土。北京中国社会科学院考古研究所藏。玉质呈浅绿色,上有褐斑。鹦鹉体扁平,呈挺身站立状,钩喙尖细,臣字形目,腹圆鼓,足上雕四爪,长尾外撇而下垂。头上有以单阴线和双钩饰纹的高冠,冠边缘有锯齿状突起。足下有榫可供插嵌。突出的高冠、尖喙和长尾使整个形象富有装饰情趣。淡绿的色调则使人联想到鹦鹉美丽的羽毛。妇好墓出土的鹦鹉共21件,以扁体浮雕为主,看似形制相像,但细部均有变化而不雷同。鹦鹉是一种美丽而乖巧的鸟,墓中出土玉鹦鹉数量如此之多,也反映出当时人们对它的喜爱。殷墟妇好墓见“殷墟妇好墓”条目。