动物胚后发育animal postembryonicdevelopment
幼体从卵壳中孵出或从母体产出后发育为成体的过程。完成胚后发育的重要标志是达到性成熟。有些动物需要经过幼虫变态阶段。这种发育称间接发育,见于纽形动物、软体动物、昆虫、棘皮动物和两栖类等; 大多数动物不需要经过变态,称直接发育。
以具有典型性和代表性的昆虫变态和两栖类变态为例。
昆虫变态 类型很多,由简单到复杂,主要可分为5种。❶无变态: 有数次蜕皮,但各龄幼虫的形态无多大变化,故又称原变态,如低等昆虫中的衣鱼、跳虫和双尾虫等变态。还有一种次生性的无变态,是由于幼虫与成虫的生活环境相似所形成,见于虱和无翅蝗等。
❷半变态: 由幼虫变为成虫时,一部分幼虫器官退化消失,另一部分则保留,如蜉蝣、蜻蜓等变态。
❸渐变态: 各龄幼虫与成虫之间无多大差异,主要变化在于各部比例和体型逐渐变大,以及单眼等器官发生等,如蝗虫的变态。以上三种变态均无蛹期发生,它们统称为简单变态或不完全变态,其各龄幼虫统称为若虫。
❹完全变态: 是典型的有蛹期的变态,可见于内翅类。其幼龄幼虫多呈蠕虫状,缺乏复眼和外翅,其翅芽埋于幼虫的角质层下到蛹期才外露; 有的幼龄幼虫有不发达的触角和胸足,或有暂时性的腹足和尾毛,还有的全部缺乏足、口器和触角等; 末龄幼虫(即蛹前幼虫) 蜕皮后进入蛹期,变成的蛹常在围茧内不吃不动,同时体内的幼虫器官坏死分解,成体器官芽则在生长发育,变为成虫后破茧而出; 初孵出的成虫大多色灰白,翅小而皱,随后翅变硬而展开即显示成体形态,如粉蝶的变态。
❺复变态: 是一种完全变态的复杂形式,其不同龄幼虫形态各异,如芫菁的变态,它包括活动性强的柄形幼虫,变得粗大的蠋形幼虫和最后不活动的蛆形幼虫,然后进入蛹期,由蛹再羽化为成虫。各类变态都有组织分解和组织生成的变化过程,有的是纯破坏性变化或纯建设性变化,还有的是既有破坏又有新建的居间性变化,其中白细胞和巨噬细胞对组织的分解和吞噬很重要。昆虫变态过程的发生受神经内分泌系统的调控(见内分泌系统),分泌的蜕皮激素、保幼激素、促蜕皮激素和蜕皮抑制激素参与控制昆虫的蜕皮和由幼虫向成虫的变化,其中包括器官芽的发育和蛹化期的表现等。
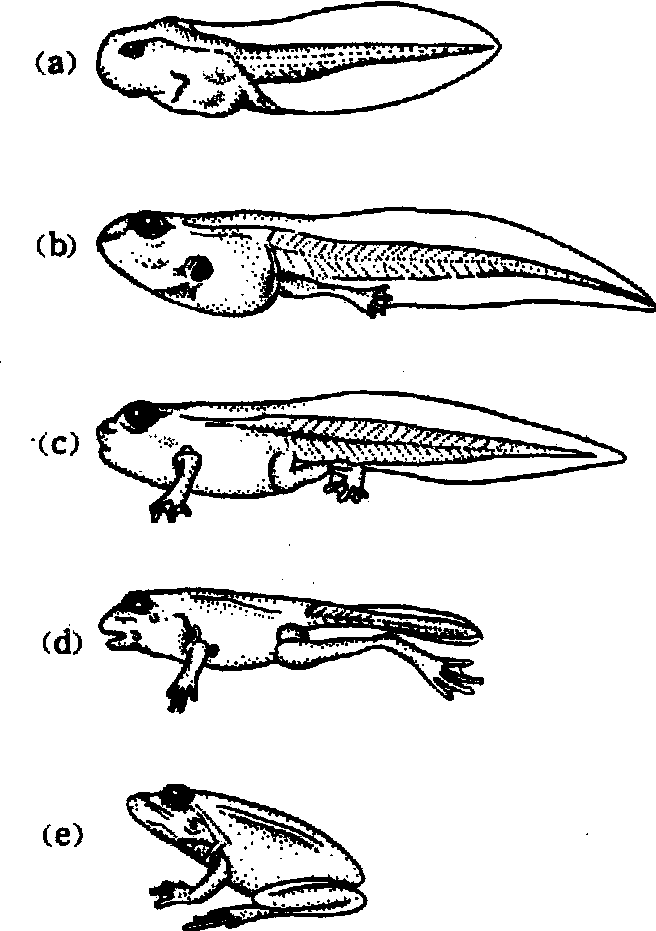
两栖类(豹蛙)的变态
(a)幼虫期; (b) 变态初期; (c) 变态顶峰初期(d)、(e) 变态顶峰期,小蛙形态形成
两栖类变态 其幼体有尾。蛙的蝌蚪形态在孵化前即已出现,孵化后经历幼虫生长期、变态初期和变态顶峰期变为小蛙(见图),再由小蛙过渡为成蛙。❶幼虫生长期:口长出角质颚和角质齿,头两侧生出鳃盖,内鳃形成,眼位于头背部两侧,无眼睑; 表皮生出许多大型色素细胞,肛门位于背方; 肺芽生出,消化管加长并盘曲。
❷变态初期:先生后肢而后前肢,鼓膜发生,眼睛变大,肛门移至体外后端腹侧。
❸变态顶峰期: 几乎全部组织器官都在发生变化,以适应将来陆生生活的需要。如角质颚脱落,口唇部长有细齿,眼球更加突出并移向背侧,眼睑生出,口变宽,颚肌发达,肉质舌生出; 尾逐渐消失,后肢不断伸长; 消化管变短,内鳃退化,肺迅速长大,舌颚骨和一些有助于空气入肺的肌肉均分化出来等。两栖类的变态受神经内分泌系统的调控,其中甲状腺素(T3、T4)直接控制蝌蚪的变态;下丘脑-垂体激素则对甲状腺素的分泌起调节作用,参与的激素有下丘脑的促甲状腺素释放因子、促乳素释放抑制因子和垂体远侧部的促甲状腺素和促乳素。