网站首页 百科知识
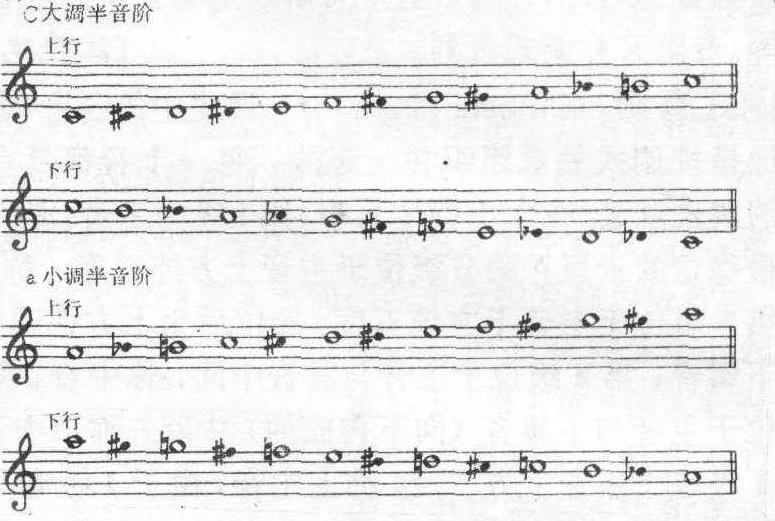
简称半音阶。音阶中相邻各音均为半音。半音音阶的记谱法一般上行时用升号。如:
开放百科全书收录579518条英语、德语、日语等多语种百科知识,基本涵盖了大多数领域的百科知识,是一部内容自由、开放的电子版国际百科全书。